The Future of Detecting Brain Damage in Football
A new technique could revolutionize how a neurodegenerative disease afflicting contact sports is treated.
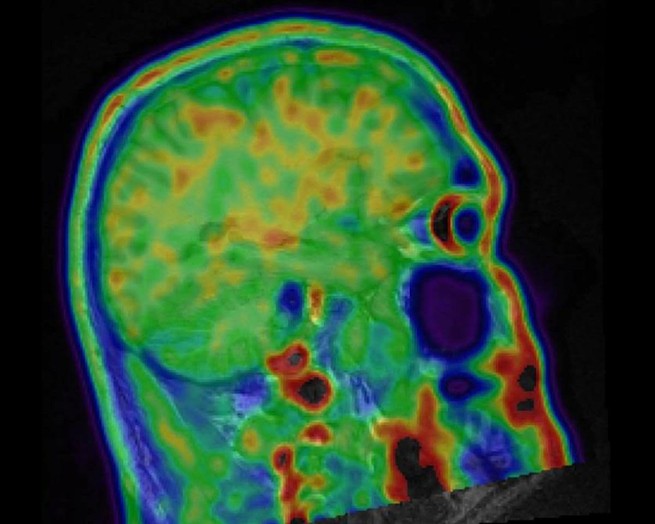
Sam Gandy had never seen anything like it. He was examining brain scans, color-coded to indicate problems. In healthy people, images appear almost entirely blue and green. But several areas on this particular scan were bright red.
Gandy, a neurologist at Mount Sinai Hospital in New York, was studying the brains of retired soldiers and football players, looking for signs of trouble like this. The scan that stood out was of a retired National Football League player who had suffered 22 concussions over the course of his 11-year career. Now approaching middle age, the player complained of memory lapses and a short fuse—symptoms associated with chronic traumatic encephalopathy, or CTE, a neurodegenerative disease linked to repetitive brain trauma.
Currently, CTE can only be definitively diagnosed after death. But the red areas Gandy saw on his computer screen closely corresponded to the damage that scientists see of the disease in autopsied brains. Gandy’s technique might be the first way to spot CTE in a living patient. If so, what he was looking at could change the future of contact sports—as well as treating the long-term damage they can cause.
Since CTE was identified in the brain of former Pittsburgh Steelers player Mike Webster in 2005, the disease has plunged football into an ongoing brain-injury crisis. A recent study of the brains of 202 deceased former football players revealed that 110 of the 111 who had played in the NFL had the condition. Athletes whose gridiron careers ended at the high-school and college levels also also had the disease, though in lower percentages. (There are limitations to this research—more on that momentarily.)
Coming on the heels of multiple studies suggesting that repeated blows to the head can be bad for the brain—and of CTE being found in soccer players, soldiers, and others—this study only intensified concerns about football: Is the sport, which kicked off another season this month, safe enough for children? For high schools? For anyone?
The fact that CTE can only be diagnosed posthumously makes answers difficult. Researchers can’t say how common the disease really is, because studies suffer from unavoidable selection bias: The brains examined aren’t chosen at random from the general population, or even the overall population of contact-sport athletes and others exposed to repetitive head trauma. Rather, most are donated for study because donors and their families suspected something was wrong.
Researchers also don’t know exactly how CTE starts—though research on concussed mice has offered intriguing clues—or how it progresses over time. They don’t understand why some people who suffer repetitive head impacts develop the disease while others don’t. Nor can they target and test potential medications and therapies.
A reliable in-vivo way to diagnose the condition, says Robert Stern, the director of Boston University’s Chronic Traumatic Encephalopathy Center, is “the goal for all research now with CTE. We’ve learned a tremendous amount through the postmortem data and research. But that’s the starting place.”
Enter Gandy. A longtime Alzheimer’s researcher, he began to study contact sport–related brain disease in the 1990s, when he coauthored a study that found boxers who had fought in 12 or more professional bouts and had a particular genotype were more likely to have chronic neurological deficits.
Three years ago, a 73-year-old retired New York Jets player with memory problems named Dave Herman wanted to enroll in a Mount Sinai clinical trial for an Alzheimer’s drug, but the five doctors who examined Herman—Gandy among them—couldn’t agree on what was ailing him. Three thought he had Alzheimer’s. Two suspected CTE. So Gandy examined Herman’s brain twice using positron-emission tomography (PET) scans—once with a radioactive tracer that binds to beta-amyloid, a sticky protein that builds up in the brains of Alzheimer’s patients, and again with a new tracer that binds to tau, a different protein that misfolds, clumps, and forms toxic tangles in the brains of CTE patients.
![Axial images of T1-weighted MRI overlaid with [18F]AV-1451/T807 PET in a healthy control (left) and in a National Football League (NFL) player with a history of 22 concussions and clinically probable chronic traumatic encephalopathy (CTE; right)](https://cdn.theatlantic.com/thumbor/WHz_woyiskp49383Tud4fzEkgs4=/0x0:1280x709/655x363/media/img/posts/2017/09/sidebyside/original.jpg)
The first scan came back negative. The second was positive. Herman likely had CTE. Only doctors couldn’t be entirely sure; the scans were lacking in detail, and scientists hadn’t agreed on a postmortem diagnostic standard for the disease, so Gandy couldn’t match with full confidence what he saw in Herman’s scan to the tau tangles seen in the autopsied brains of CTE patients. A year later, however, an expert panel commissioned by the National Institute of Neurological Disorders and Stroke, or NINDS, agreed on what distinguishes CTE from other diseases that also feature tau deposits: In CTE, the neuron-killing protein tangles build up around the wrinkled crevices along brain’s surface, particularly at the deepest points.
Armed with that definition and higher-resolution scans, Gandy was better able to tentatively diagnose the retired NFL player who had suffered 22 concussions, and who also showed neuropsychological testing deficits and diffuse brain damage through separate MRI scans. (The player discussed Gandy’s findings with The Atlantic, but requested anonymity because of the stigma associated with brain injury.) “With the better resolution in the [PET] scans, we could see the localization of the tau in exactly that spot, the bottom of the walls of the wrinkles,” Gandy says. “It looked very similar to what you would expect from a postmortem [CTE] brain.”
Since then, Gandy’s team has examined and scanned almost 30 combat veterans and former football players. Ten of those patients have clinical symptoms of CTE; of that group, eight have what Gandy describes as “clearly positive scans” for abnormal tau buildup, similar to that of the NFL retiree. The other two “may not have accumulated enough tau for us to see it yet,” Gandy says.
Before PET scans can be used to definitively diagnose CTE—or simply be used with a high degree of diagnostic confidence—more work needs to be done. A handful of cases are suggestive, but not conclusive; many more patients need to be scanned, evaluated by doctors, tracked over time, and eventually autopsied after death to validate the bright-red regions Gandy and his team are seeing on their computer screens. “That’s the gold standard,” Gandy says. “It will take a while to accumulate enough data to feel confident that a certain amount of signal represents a certain amount of tau.”
A number of tau tracers have been developed in recent years, and researchers are still figuring out which ones are the most useful for identifying various neurodegenerative diseases. Two years ago, researchers at the University of California, Los Angeles, published a brain-imaging study of 14 former football players using a tracer called FDDNP to identify what appeared to be CTE. But that same tracer also binds to amyloid, making it difficult to differentiate the disease from Alzheimer’s.
Gandy uses a compound called Flortaucipir, which binds much more readily to tau than to amyloid. But he cautions that it may not prove to be the best available imaging agent. “Most people who get the scans want a definitive result,” he says. “But we always tell them this is experimental, and we could find out something tomorrow that changes things. ”
Better answers may come from a recently announced seven-year, $16 million study funded by the National Institutes of Health and NINDS that’s aimed at diagnosing CTE—a project the NFL was also slated to fund before backing out amid controversy. Headed by Stern, the project is the largest and most thorough study of the disease ever conducted, and will put former football players through a series of tests including an MRI; two PET scans; blood, saliva, and spinal-fluid collection; genetic evaluations; neuropsychological testing; and clinical examinations and histories.
The goal, Stern says, is to create a reliable clinical tool kit—that is, multiple methods of diagnosing CTE, similar to how doctors detect prostate cancer by using relatively cheap and simple blood tests to determine which patients need more thorough examinations. “PET scans are really good, but are also are really expensive,” he says. “We need other ways of detecting CTE that are really good and less expensive, or not really good and less expensive.”
Stern believes that doctors will be able to diagnose the disease in the living within five years. If and when that happens, it will allow researchers to better study potential treatments. In particular, PET scans may enable them to see if a drug is working. Sometime in the next year, Gandy’s team hopes to have the tau-positive patients from its imaging study participate in a small clinical trial of a new medication that has shown the ability to repair and clear out misfolded tau in animals.
“Once someone has the symptoms of a neurodegenerative disease like CTE, it usually means that there is already damage to the brain, destruction of tissue and atrophy. We can’t get those cells back once they die,” Stern says. “If we see [the disease] early enough, we might be able to intervene in a way that slows down or even stop the disease progression.”
The ramifications for contact sports—especially football—could be equally profound. Youth football participation is declining, and a number of college and NFL players have walked away from the game, citing concern over brain injuries. It’s not hard to imagine someone like Gandy giving brain scans to entire high-school, college, and pro teams. The results might restore confidence in the overall safety of the sport—or further erode it.
“Every fall, I read how fewer and fewer kids are coming out to play high-school football,” Gandy says. “With scans, we could figure out what the risk really is. And we could have informed consent for people who want to get into this kind of activity—be able to say that you have a one in 100, or 1,000, or 1,000,000 chance of getting CTE. But we need to get to the point where every doctor can look at an image and say, ‘that is CTE, no question about it.’ Otherwise, it would be a mess.”